A GUIDE TO BREAST IMPLANT COMPLICATIONS
– NEWPORT BEACH, CA –Though breast implants can help you attain the breast appearance you desire, it’s important to appreciate that your breast implants are not permanent and may require replacement during your lifetime.
Plus, several problems may arise as a result of using implants. These may occur soon or many years after your breast augmentation.
Familiarize yourself with the possible complications of getting breast implants so that you can make an informed decision before your plastic surgery.
Read on to find out more.





What are Breast Implant-Related Complications?
Breast implants are human-made devices created by three USA manufacturers: Allergan, Mentor, and Sientra.
Although breast implants are extremely safe and used by about 350,000 patients annually in the US, they are not without their own set of related issues and problems. Like any other human-made implantable medical device (such as heart valves and artificial joints), some patients will require revisions or reoperations.
Before and After
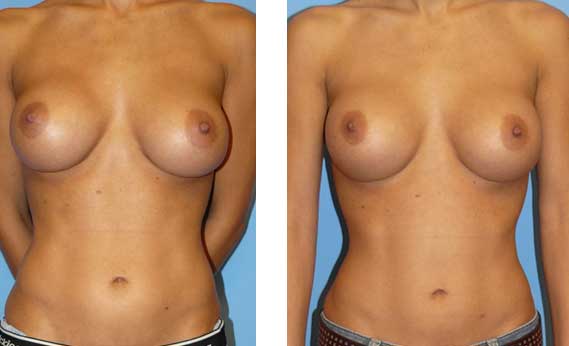
This is a 27-year-old female who exchanged her saline implants with silicone implants and had her right nipple asymmetry corrected by Dr. Agha.
The post-operative picture was taken at one year.
Dr. Siamak Agha of The Aesthetic Centers uses a systematic approach to breast augmentation, minimizing implant-related complications while improving patient outcomes and satisfaction ratings. He feels that the real focus should be on the prevention of these problems as much as possible.
Still, it won’t hurt to know about these possible complications, which are as follows:
Capsular Contracture
Capsular contracture is the leading cause of breast augmentation complications. It occurs when the scar tissue or capsule that usually forms around the implant tightens and squeezes the implant.
This can cause the implant to migrate or get displaced, resulting in a tight-looking and deformed breast. It can also be painful.
Capsular contracture happens over time in one or both of the implanted breasts. It may be more common following infection, hematoma, and seroma. Plus, the chances of it happening may increase over time.
Capsular contracture is believed to be caused by contamination of the implant with bacteria normally residing in breast glands. The bacteria form a biofilm around the implant to which the human body reacts by thickening the usually paper-thin capsule.
Symptoms of capsular contracture range from mild firmness and mild discomfort to severe pain, distorted shape of the implant, and palpability — the ability to feel the implant.
Before and After
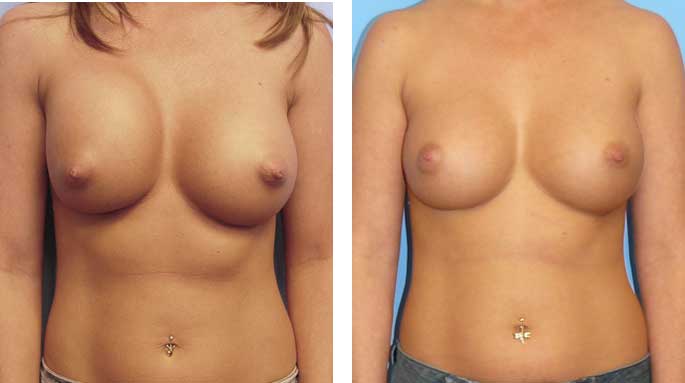
This 31-year-old female developed capsular contracture about four months after her submuscular breast augmentation with saline implants.
The patient underwent a complete capsulectomy and implant exchange by Dr. Agha six months after her first surgery.
The post-op picture is shown three months after reoperation.
Breast Implant Rupture or Deflation
Breast implants rupture when the implant shell develops a tear or a hole.
Rupture may occur any time after implantation, but they are more likely to do so the longer it is implanted.
According to a study by the Institute of Medicine, the following procedures may contribute to breast implant rupture or deflation, which is why Dr. Agha strictly avoids them:
- Closed capsulotomy, a technique used to relieve capsular contracture that involves manually squeezing the breast to break the hard capsule
- Placement of drugs or substances inside the implant other than sterile saline
- Injection through the implant shell
- Alteration of the implant
- Stacking of the implants, which happens when more than one implant is used per breast pocket
Other reasons for the rupture or deflation of breast implants include:
- Normal aging of the implant
- Damage caused by breast procedures, such as biopsies and fluid drainage
- Significant compression during mammographic imaging
- Stresses, such as trauma or intense physical pressure
- Capsular contracture
- Under-filling of saline-filled breast implants
Dr. Agha recommends removing the implant if it has ruptured, regardless of whether it is saline-filled or silicone gel-filled.
Before and After
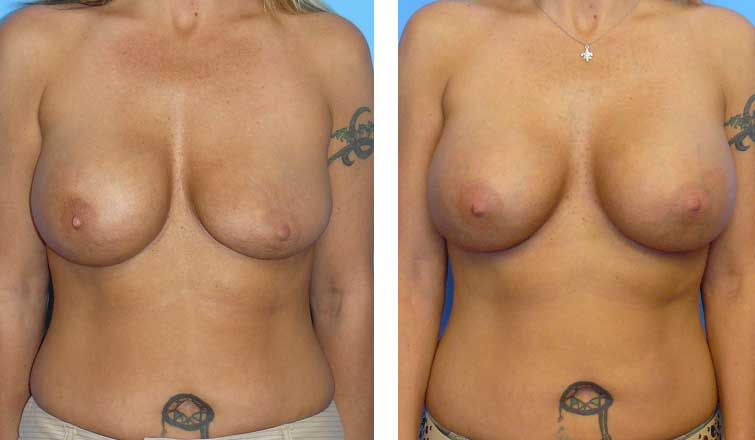
The patient underwent an exchange of both saline implants.
The post-op picture is shown three months after reoperation.
Implant Rippling and Implant Show
Most breast implants ripple. However, this becomes a problem when implants are placed in a subglandular pocket in a thin person who does not have enough breast tissue to cover the implant.
The rate of implant rippling and show is lower when the implant is placed under the chest muscle. It is also less likely to happen when a silicone implant is used.
Read more about implant rippling here.
Breast Pain
About 5% to 15% of women may feel breast pain of an unknown cause following breast augmentation. Wrong size, placement, surgical technique, and capsular contracture are just some of the possible reasons why you experience breast pain.
Removal of the implant has been shown to improve pain in some patients. Make sure to tell your doctor if you experience any pain post-breast augmentation.
Breast Implant Illness
Breast implant illness (BII) refers to a wide range of symptoms that might develop after breast augmentation or breast reconstruction surgery.
To learn more about BII, proceed to this blog post.
BIA-ALCL
BIA-ALCL stands for breast implant-associated anaplastic large cell lymphoma — a rare type of cancer associated with Allergan’s textured breast implants.
Although related to breast implants, it is a cancer of the immune system and is associated with the implant capsule.
Though it is rare for this type of cancer to metastasize, some patients choose to undergo implant removal as a preventive measure or treatment.
Get Your Breast Augmentation Done in Orange County and Los Angeles
When selecting a plastic surgeon to perform your breast augmentation, it is important to understand their complication and re-operation rates and choose a board-certified plastic surgeon who can deal effectively with any complication.
Fortunately for you, Dr. Agha fits the role well. His reoperation rate is significantly lower than those published in the plastic surgery literature.