CHEST ENHANCEMENT
– CHEST LAXITY AFTER MASSIVE WEIGHT LOSS –The chest refers to the area that covers the rib cage in the front. It typically spans from the collar bones (clavicles) all the way to the 12th rib and is separated in the midline by the breast bone (sternum) to left and right chest. The chest area can be arbitrarily broken down to the breast area, upper chest above the breast, lower chest below the mammary crease and the outer chest on the sides.
Following weight loss, the fatty layer under the skin as well as the fat within the breast undergo shrinkage. This results in redundancy of the chest skin as well as breast skin envelope. Redundant excess chest skin is seen as horizontal and vertical laxity. Horizontal chest laxity causes skin and tissue excess under the armpits and over the outer chest. Vertical chest laxity affects mainly the breasts, causing breast sagging in both men and women.
However, when the degree of weight loss is significant, vertical chest laxity presents itself as breast mound descent on the rib cage and loose mammary crease attachments.
The loose tissue may also create a fold under the breast and over the upper abdomen. This tissue roll typically stretches towards the back and join the upper/ midback rolls. This is particularly common in V-shaped body structures where the upper body is larger than the lower body.
In both men and women, breast deflation and sagging (breast ptosis) develops. These are classified according to the degree of severity in both genders.

Grades of Breast Sagging in Females
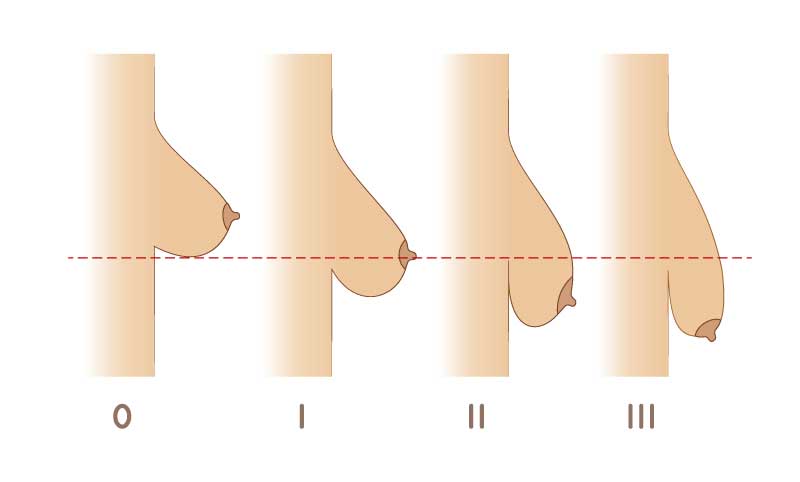
In women, there are 3 grades of breast ptosis, dependent on the severity of breast sagging. To learn more, please visit our breast enhancement page.
- Grade 1 – characterized by mild sagging as the nipple lies at the level of the inframammary fold and the parenchyma below it
- Grade 2 – characterized by moderate sagging as the nipple lies below the level of the inframammary fold but above the lowest hanging part of the parenchyma
- Grade 3 – characterized by severe sagging as the nipple lies way below the level of the inframammary fold at the lowest hanging part of the parenchyma
Types of Gynecomastia in Males
Similarly in men, there are 4 types of gynecomastia. These are summarized in the table below.
| Type | Activity |
|---|---|
| 1 | A localized button of breast tissue under the areola |
| 2 | Moderate enlargement of breast tissue exceeding boundaries of areola and indistinct from the chest |
| 3 | Moderate enlargement of breast tissue exceeding boundaries of areola and indistinct from the chest with skin redundancy |
| 4 | Marked enlargement of breasts with significant skin redundancy and feminization of the breasts |
Weight loss patient’s typically present with grade 3 breast ptosis in women and type 4 gynecomastia in men.
The problem with the gynecomastia classification is that it focuses on the breast only and does not consider the rest of the chest.
That is why Dr. Agha designed his own chest deformity classification that focuses on the whole chest as an aesthetic unit. It also puts the spotlight on the two elements that need to be addressed in chest enhancement surgery: excess skin and excess fat or breast tissue.
Dr. Agha’s Chest Deformity Classification:
Correction of Chest Laxity And Breast Sagging

Most weight loss patient’s typically present with Agha’s Chest Laxity Classification type 4 or 5. That means in addition to breast sagging (in both men and women), they also have outer chest and lower chest tissue excess.
To tackle these changes, a number of procedures have been described by Dr. Agha and other plastic surgeons.
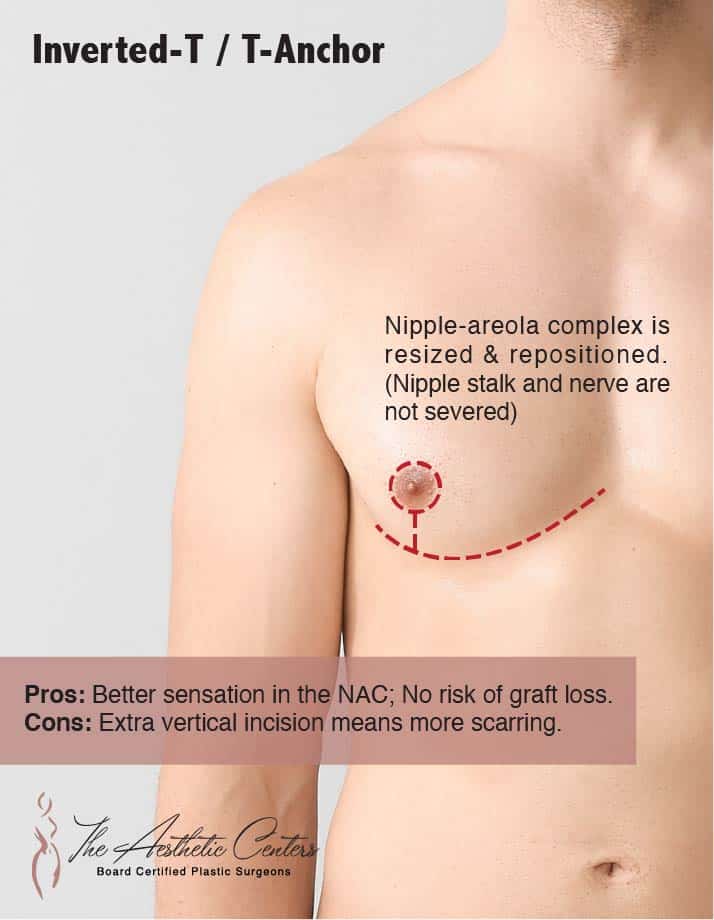
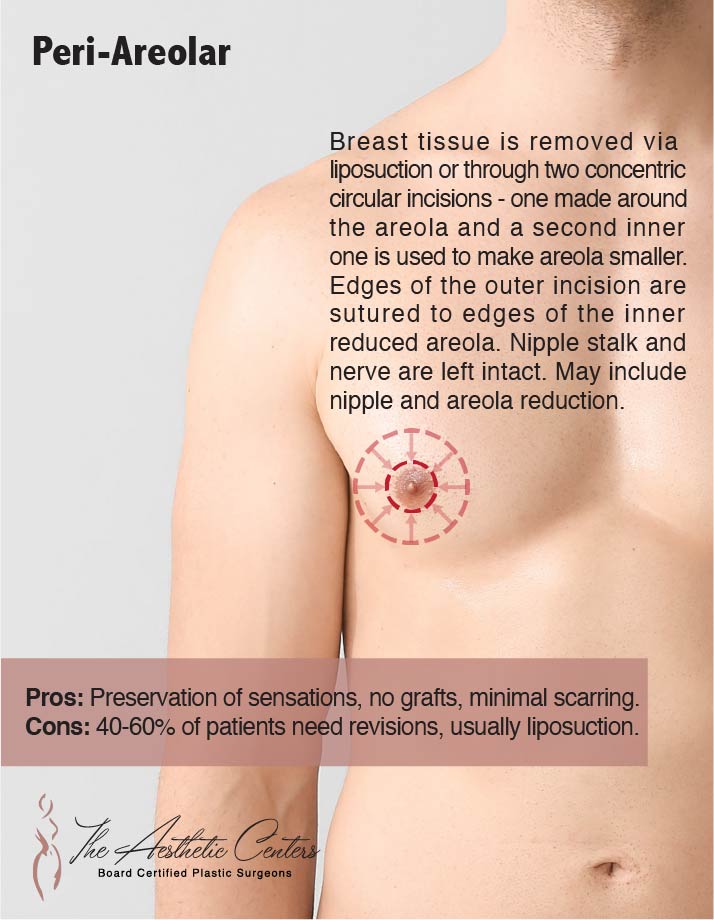
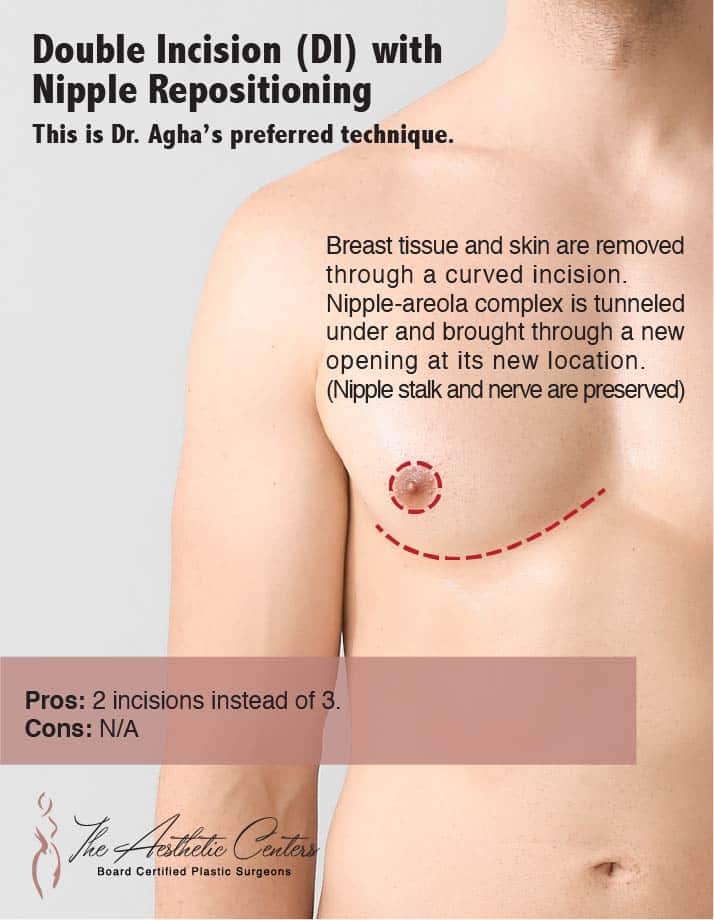
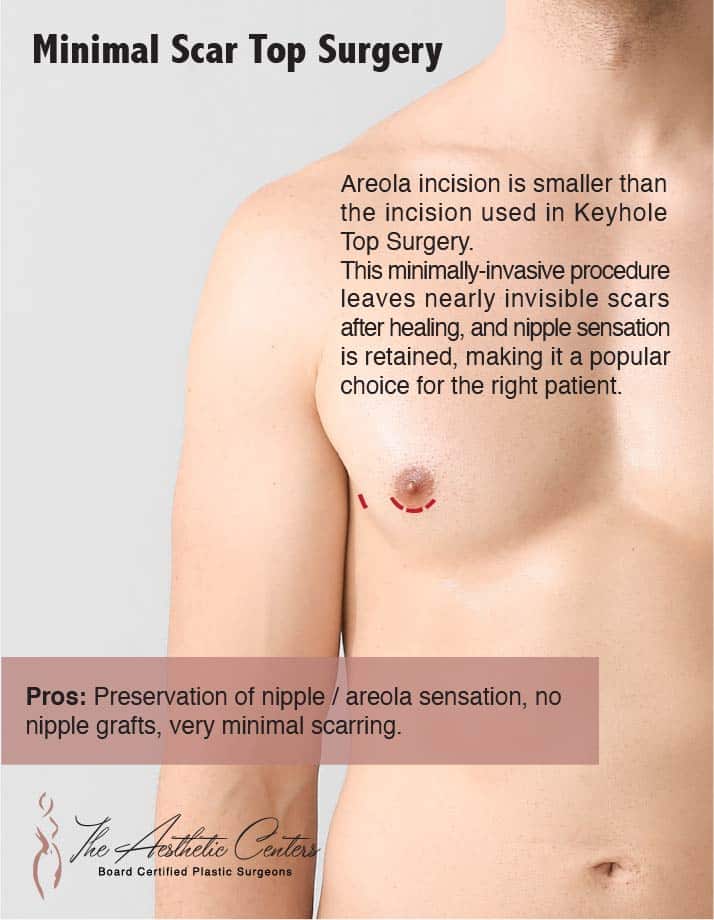
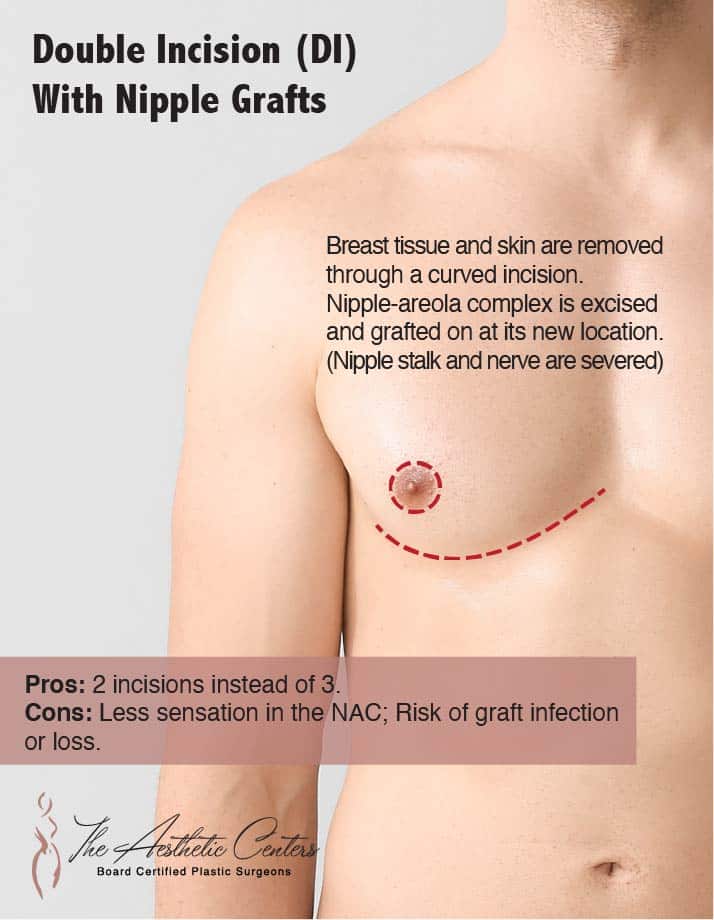
In men with gynecomastia (excess breast gland), a horizontally-oriented elliptical excision of excess breast can lift the nipple areola on the chest while removing the excess breast tissue. Alternatively, the patient may end up with a curved incision at the breast crease, an anchor-type incision, or a horizontal incision on each side of the nipple areola. To learn more, please read our gynecomastia section.
In women with breast sagging, in most cases, an anchor-type incision is needed to remove enough skin to lift the breasts and to make them rounder. This can be combined with breast implants, breast reduction, or neither. To learn more, please read our breast surgery section.
For lower chest excess below the breasts as a roll of redundant loose skin, a reverse tummy tuck can be combined with the elliptical or anchor-type incisions excision to remove the additional skin laxity and to produce a smooth and tight chest contour.
For excess outer chest skin, a vertically-oriented elliptical excision below the armpit, removes excess outer chest skin. This procedure was pioneered and named the J-upper body lift by Drs. Agha and Hurwitz.
Dr. Agha’s Male Chest Deformity Classification and Approach to Chest Enhancement
| Dr. Agha’s Classification | Features | Treatment |
|---|---|---|
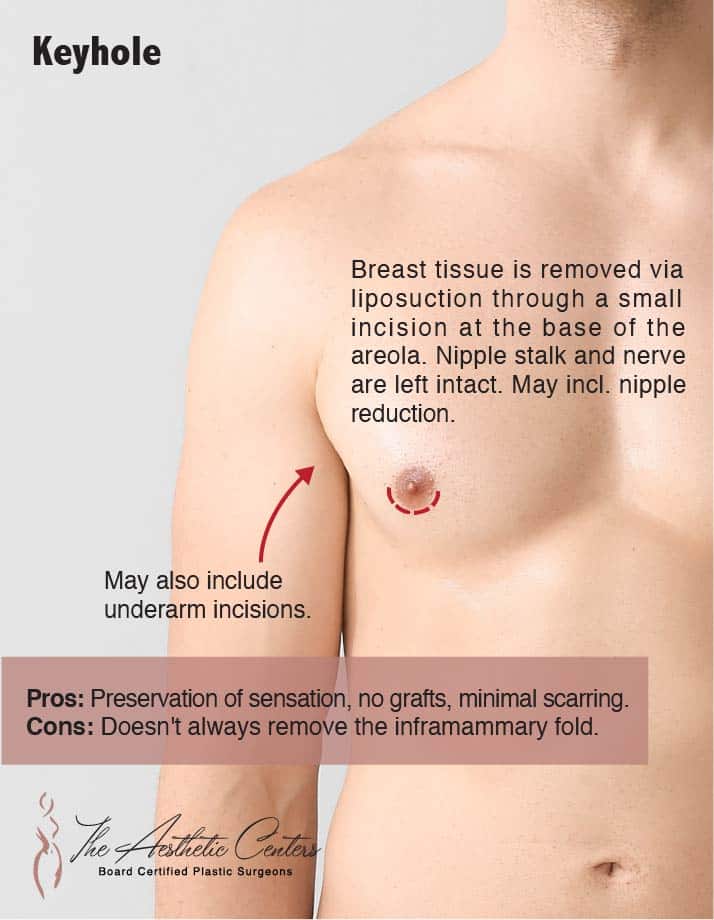
| Type 1 | -Minimal chest skin laxity -Good skin quality with excess breast tissue -May or may not have excess fat | -Liposuction for fat removal -Periareolar incision for breast gland removal |
| Type 2 | -Mild to moderate degree of chest skin laxity -Good skin quality with excess breast tissue and fat | -Liposuction for fat removal -Periareolar incision for breast gland removal |
| Type 3 | -Marked chest skin laxity -With hanging breast (vertical skin laxity) | -Horizontally-oriented elliptical excision for excess gland, skin, and fat removal |
| Type 4 | -With hanging breast (vertical skin laxity) -With outer chest skin excess and bulge (horizontal skin laxity) | -Horizontally-oriented or Anchor-type incision to excise gland, skin, and fat -Vertically-oriented elliptical excision below the armpit to remove excess outer chest skin |
| Type 5 | -With hanging breast (vertical skin laxity) -With outer chest skin excess and bulge (horizontal skin laxity) -Bulging lower chest skin | -Horizontally-oriented or Anchor-type incision to excise gland, skin, and fat -Vertically-oriented elliptical excision below armpit to remove excess outer chest skin -Reverse tummy tuck |